
Children and Families - Single Assessment Protocol and Guidance
Scope of this chapter
This chapter details the process of the Single Assessment, highlighting its purpose, the thresholds to consider whilst undertaking one and the issues to be explored. Emphasis is made on ensuring the child is seen and their views, (where appropriate) are obtained. The chapter highlights questions that practitioners and managers should seek to address and include as an outcome in their evaluation. Additional source material is identified.
Related guidance
The Single Assessment was introduced to Bolton in September 2013 as a pilot in response to Eileen Munroe recommendations and revised Working Together to Safeguard Children. The single assessment is named the Children and Families Assessment in Bolton.
The new framework for Single assessment replaces the old system of initial and core assessments. The guidance allows Local Authorities to develop their own assessment framework and timescales for assessment. Albeit Working Together guided that assessment should be no longer than 45 days.
Munro’s aspirations for the removal of timeframes were to provide opportunity for social workers to focus on the specific needs of and allow appropriate time within assessment for reflection and direct work with the child/young person to ensure robust and analytical assessment. Allowing professional autonomy, and ability to draw on professional judgement to analyse and reflect on information gathered regarding that child or young person, and focus the assessment ensuring it is child centred.
Working Together (archived) 2013 communicates a clear aim of the revised framework for assessment:
“The aim of the new Children and Families Single Assessment Form is to retain the Framework for the Assessment for Children in Need and their families (Department of Health and Social Care (DHSC) et al.: 2000) as an underpinning framework and examine children's developmental needs, parents or care givers capacity to respond appropriately and family and environmental factors which are specific to the purpose of assessment for that child. However the form is able to be streamlined so that there are fewer tick boxes ‘ and/or sub - sections for each of the dimensions (e.g. health, education, emotional, and behavioural development) of the Assessment Framework to encourage and empower social workers to exercise their professional judgement about what information to record”
It is expected that changes to cultural practices around undertaking and approaching assessment will take some time. However the immediate aims of the single assessment are to:
- Reduce prescriptive, tick box style assessment;
- Allow greater opportunity for the social work practitioner to engage with children to explore their wishes and feelings focusing upon the child’s journey and the impact of the concern upon their safety and wellbeing;
- Increased opportunity for practitioner to reflect upon the assessment and greater emphasis on social work accountability;
- Greater focus on analysis and impact on the child;
- Opportunity for it to be seen as specialist assessments (e.g. court reports).
With increased timescales, however, comes the risk of delay and drift in managing workflow through front door services. It is expected that by day 15 the social worker will have arrived at a conclusion regarding the outcome of an assessment and intervention. The key tasks of seeing the child/children, and discussing issues with key family members will have been considered. Key tasks such as researching history and key agency information are essential to effective assessment.
Drift and delay will be managed stringently by the Team Manager. Assessments should not be reset to 45 days due to worker capacity to complete an assessment within 15 days. Triggers for 45 day assessments will be discussed later.
The purpose of assessment is to gather information and evidence about a child and their family to identify whether a child is a Child In Need (Section 17) or whether the child is at risk of suffering or likelihood of suffering Significant Harm (Section 47). An assessment is not an end in itself but the means of informing the delivery of effective services for children and families. This can only be delivered if the assessment has been holistic and smart effective planning runs alongside it.
The need to assess can also include pre-birth situations when a mother's own circumstances would give cause concern that the pre-birth, and then born, child would come within the definition of being a 'child in need' (see Section 4.1, Pre-birth 'Good Practice Steps').
An assessment must be carried out by a qualified social worker, or a student Social Worker under supervision of a Qualified Social Worker. The assessment must be based on a sound knowledge of child development and be seen in the context of the child’s family and environment. The social worker leads the assessment, which must be informed by the child and their family members and by other professionals who know them, including teachers, health visitors, and relevant key agencies. The overall aim of assessment should be to determine the level of need and or risk by ensuring a clear, robust and succinct analysis of the child and family, and any key issue and impact that they may have on children's outcomes. The assessment must be completed in a timely manner, making decisions in the best interests of children, and within a timescale which has the child’s safety as its paramount concern.
Should this risk or need be evident, the assessment should then recommend what is to happen next and outline a plan of action; ensuring any suggested plan is smart. Should the analysis of the case lead to closure - clear rationale is needed in relation to this and consideration given to step down processes and lead professional roles where necessary.
It is essential that the child remains the focus of the assessment, to the extent of identifying needs and the impact of parenting capacity and wider community influences. For instance the needs of a parent may evidence issues of alcohol, emotional or mental health problems, their lifestyle may be affected by domestic violence and abuse or substance misuse, and all these issues need to be considered in respect of the impact on the child.
The child/children should be seen within 10 days of the referral. This should be made explicit in social workers practice. If a child has not been seen by day 10, this should be raised with the Team Manager to review the case and intervention. Team Managers have an explicit role in ensuring children are seen in a timely fashion and must stringently ensure this practice. No assessment should be authorised without a child being seen.
The focus of single assessment will follow the domains of the Framework for Assessment triangle as illustrated in the diagram below:
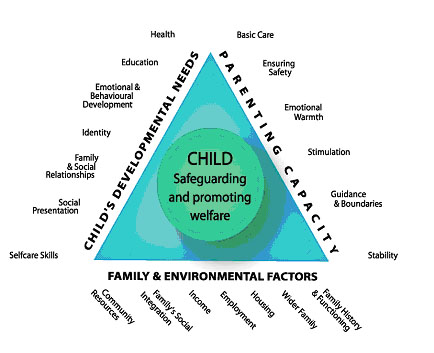
In considering the domains of the assessment framework, a clear and succinct analysis of risk has to be considered. It will be expected that social workers link analysis to research and the use of wider assessment tools to ensure evidence based assessments. These tools should be made explicit within the assessment. For instance if the graded care profile had been used then it should be made explicit within the analysis how this has been used and the evidence it has produced relating to the impact of the child.
It is essential that the assessment includes and reflects the wishes and feelings of a child. The child needs to remain the focus of the assessment; the analysis should explain impact of key issues on the child’s wellbeing. A day in the life tool should always be considered when undertaking an assessment with a child.
No assessment should be undertaken without the inclusion of the key family members. Careful consideration should be considered when it comes to engaging families and use of appropriate challenge. Assessment should not just focus on a critical incident but consider and ensure key history and previous referrals, wider agency information is gathered and analysed. Communication with families is essential, families must understand the purpose and focus of the assessment and assessments should always be shared with families.
Assessment will also include all the relevant key agencies, such as education, health, police, etc. It is essential a holistic picture is built of the family and child to inform outcomes and analysis.
Whilst undertaking assessment is crucial, it is recognised that professional can fall privy to pitfalls and barriers. Working Together (archived) 5.11.3 stresses that "The balance needs to be struck between taking action designed to protect the child from abuse whilst at the same time protecting him or her and the family from harm caused by unnecessary intervention".
- Pressures from high status referrers or the press, with fears that a child may die, lead to over precipitate action;
- Professionals think that when they have explained something as clearly as they can, the other person will have understood it;
- Assumptions and pre-judgements about families lead to observations being informed or misinterpreted;
- Parents behaviour whether cooperative or uncooperative, is often misinterpreted. Tokenistic engagement at times is accepted;
- Not enough weight is given to information from family, friends and neighbours;
- Not enough attention is paid to what children say, how they look and how they behave;
- Attention is focused on the most visible or pressing problems and other warning signs are not always appreciated;
- When the initial enquiry shows that the child is not at risk of suffering or likelihood of suffering significant harm, families are seldom referred to other services which they need to prevent longer term planning - not enough effective use of step down processes;
- When faced with an aggressive or frightening family, professionals are reluctant to discuss fears for their own safety and ask for help leading to professional avoidance;
- Information taken at first enquiry is not adequately recorded, facts not checked and reasons for decisions are not noted.
Hedy Cleaver, Corinne Wattam, Pat Cawson, Rosemary Gordon.(1991)
Ten Pitfalls and How to Avoid Them. What Research tells us.
NSPCC
The aim of single assessment frameworks is to also ensure a single planning process for a child. Active planning at the earliest opportunity should identify and put in place services or interventions which will deliver the right help to children and families at the right time. A combined assessment and planning process should develop a robust understanding of the child’s journey to date and evidence the impact of existing plans in place at the point of referral. The use of chronologies should inform planning, interventions and the approach to assessment. Early planning will complement and inform a process of robust assessment, but changes in circumstances should, prompt a proportionate review of current interventions and not lead to an 'open ended' assessment. Professional judgement and management oversight should identify when reassessment or a change in plan should be triggered.
With the introduction of the Public Law Outline (PLO), frontloading of assessments has identified the need to be as thorough and holistic as possible from the onset of an assessment. These assessments serve a crucial purpose for planning for children. The child's lived experience should be evident within the assessment. The early assessment will contribute to eventual permanency planning for a child in some cases, therefore gaps in assessment information can interrupt effective planning, and either cause delay or weak decisions for children in planning appropriate longer term plans.
On receipt of a contact to Children’s Social Care, the Multi-agency Screening and Safeguarding Service has 24 hours in which to make a decision about any actions to be taken. A contact may proceed to a Referral.
If a decision is made that a referral requires an assessment, the allocated duty worker will progress the case to 15 day assessment or extended to a 45 day assessment due to complexity. There should be a general oversight of the referrals coming through onto duty by the deputy/team manager to ensure appropriate thresholds are being met on receipt of referrals and decision making.
If safeguarding concerns are identified at the single assessment stage, a Strategy Discussion should be held to determine if a Section 47 enquiry should be progressed. It may be at this stage the priority for single assessment is reset to 45 days, via case management discussion with the deputy/team manager.
Dependant on the outcome of the Section 47 enquiries, the single assessment will either form the basis of the social workers evidence to a Child Protection Conference or child in need intervention. In either case the need for robust multi-agency planning and review is critical to the effectiveness of the process.
If at the point of referral a decision is made within 24 hours that an assessment is not required, then the referral can be closed down. However it must be made explicit, the reasons and evidence why the referral was not progressing to assessment, and decision overseen by deputy/team manager.
It will be clear at the point of referral that some assessments will require a 45 day assessment, due to the complexity of the case or the history may depict previous referrals of a similar nature.
45 Day Assessment should always be completed when:
- A Section 47 enquiry has been initiated (including in the case of concerns for an unborn child);
- The child has become Looked After;
- The child is subject to Care Proceedings;
- In the manager’s professional judgement, a 45 Day Assessment is required.
Circumstances in which the manager should always consider a 45 Day Assessment include when:
- An existing plan to meet the child’s needs is not achieving the desired outcomes;
- There have been a number of Referrals or previous assessments completed in respect of any child in the family in the previous 12 months;
- Complex Child in Need cases, where the Assessment concludes that social work intervention is likely to be required in excess of three months.
In a High Court judgment (Nottingham City Council v LW & Ors [2016] EWHC 11(Fam) (19 February 2016)) Keehan J set out five points of basic and fundamental good practice steps with respect to public law proceedings regarding pre-birth and newly born children and particularly where Children’s Services are aware at a relatively early stage of the pregnancy.
In respect of Assessment, these were:
- A risk assessment of the parent(s) should ‘commence immediately upon the social workers being made aware of the mother’s pregnancy’;
- Any Assessment should be completed at least 4 weeks before the mother’s expected delivery date;
- The Assessment should be updated to take into account relevant events pre - and post delivery where these events could affect an initial conclusion in respect of risk and care planning of the child;
- The Assessment should be disclosed upon initial completion to the parents and, if instructed, to their solicitor to give them the opportunity to challenge the Care Plan and risk assessment.
Key issues to consider when conducting the assessment
- Establish the purpose and focus of the assessment;
Following questions should be considered: why the assessment is needed, what should be the focus, what are the key issues? - Ensure where a child or family’s first language is not English the use of an interpreter;
- Key agency representation is essential and should be reflected within the assessment;
- Previous referrals, social care history, and agency history information must be considered and the current referral should not be seen in isolation of history and patterns;
- A child must be seen no later than 10 working days in receipt of the referral. Social workers must take accountability and prioritise the urgency of children being seen, given we are working with the most vulnerable children. It is good practice that every child should be seen within 3-5 days on receipt of a referral. Where children are making allegations or where there are suspicions of abuse/significant harm, children should be seen on the same day or as close to the referral as possible. This should be directed by the team/deputy manager;
- Consent to see and speak to children should always be gained, unless by doing so is likely to put the child at further risk of harm;
- Only qualified social workers can undertake assessments. Student social workers are able to undertake assessments, but under the direct supervision of a qualified social worker;
- Analysis must take account of the level of risk and identified strengths. It must evidence clearly any impact on the child;
- The child must be central to the assessment; it should clearly acknowledge the child’s world and voice. A day in the life tool should always be considered where appropriate, alongside other direct work tools where necessary;
- Chronologies must be considered and updated as part of any assessment;
- On conclusion of the assessment, recommendations must be made regarding any outcomes. Outcomes should be evidence based, therefore if concerns are identified and further action required this should be reflected in the analysis. There should then follow a plan of intervention required which may include step down processes, if social care are not going to be the lead agency. Should the assessment indicate there is no further action required, there must be explicit evidence and clear analysis as to how the concerns have reduced;
- Cases open to Safeguarding Teams and LAC Teams, assessments should be updated every year, or where there has been a critical incident;
- The Assessment Framework should guide the children and families’ assessment. Each area of need should be considered;
- 8 Assessment Practice Standards: A practice development guide to understanding children’s needs and family situations should be used and considered during every assessment;
- Abbreviations should be avoided within the assessment itself or explained;
- Copy and pasting information should be avoided;
- Consider the Early Help assessment as your baseline.
Health: To include a general overview of the child’s physical and emotional health. Contact with key health professionals such as health visitors, school nurses, other specialist workers will assist in producing an overall picture of whether the child has needs in this area. The worker should have a sound knowledge of child development to be able to comment on whether children are attaining developmental milestones, and should be led by key professionals in this area. Are appointments kept, are there specialist services involved, diagnosis or on-going assessments. Consideration must be given to use of any drug or alcohol related issues, smoking and sexual health. In more comprehensive assessments, consider where the child was born, was the child premature, what was the child early health experiences like. What were the child’s routines, sleep, and appetite?
Education/Early Years Provision: Are children attending school, achieving educationally. How is their behaviour, learning and attitude described in school. Do they require any support; have a Education, Health and Care Plan, or education plan. Pitfall is to report that are at achieving level 4 …what does this mean, be explicit, the information must make sense to the reader. Is attendance regular? If reduced how does this impact on their ability to achieve? Are they ready for learning in the morning or tired? How is education reinforced at home? Are there toys, books available for young children? Are parents able to offer a stimulating, learning environment at home in a child’s earlier years? What is the child’s education history? Do not just report on the here and now, if they are in high school where did they go to primary school, changes in education. Did they attend preschool? Do they attend groups outside of school, mosque, sports, music clubs etc.?
Emotional and behavioural development: This should be considered in relation to the degree of resilience or vulnerability of the child. What are the sources of the child’s resilience and are these age appropriate? Are they a resilient child? Does the child seem to be emotionally secure and attached? Has the child witnessed domestic violence and abuse and how does their behaviour reflect this? Consider the impact of Physical and Sexual Abuse upon the child’s behaviour and emotional presentation. Does the child feel supported and do they have a supportive adult available to them? Does the child present with difficult or challenging behaviours? Is the parental response to challenging behaviour consistent or does it fluctuate? Does the child present with different behaviours outside of the family home? What are your observations of the child’s attachment behaviours? Any traumatic experiences for the child; Consider the impact of any significant event for the child within their life and how this has affected their daily lived experiences. Has the child witnessed arguments? Has the child witnessed anybody get assaulted? Has the child witnessed their parent have a psychotic episode or taken an overdose? Has any close relative or friend died? Has the family ever experienced homelessness? Has there ever been a domestic fire? Has the family experienced burglary? Has the child had to go to hospital? Has the child been exposed to abuse?
Family and social relationships of the child: This should be considered in a way that describes what the family and their wider social circle means to the child. What is the quality and extent of child’s attachment to their caregivers and wider family? What style of attachment is evident? What’s the child’s role and involvement in this family; how are they valued and how is this demonstrated to them? Is the child taking on inappropriate responsibility within the family environment - i.e. is the child a young carer? Consider the number of care arrangements for the child; different households for some of the week? Describe the family giving a sense of their history, culture and values. Is the family a source of support and resilience? Has the family faced any traumatic or distressing events and how has this had an impact for the child? Does the family feel part of a community? Are there significant friends or organisations? Is the child involved in any gang related activity? Is the child reporting any evidence of domestic abuse that involves verbal abuse? What is the child’s peer relationships like and do they value their close friends.
Identity and social presentation of the child: Consider within this section whether the child is a valued member of the family and how is this evidenced? Does the child have access to their own private space? What are their sleeping arrangements and are their appropriate? What is a typical day? Do they have a sense of belonging? Do they participate in any organised social activity outside the home and school? Who are they mixing with socially and is this appropriate? Do parents know where they are going and is this age appropriate? Is anyone bullying the child or is there anyone the child is frightened of? Is their clothing clean and appropriate? Does the child have any friends they see regularly? Do they have a best friend? Has the child been involved in offending? Does the child demonstrate appropriate stranger awareness? Does the child recognise their ethnicity in relation to their identity? Are there any language barriers that the child faces? Is the specific child’s race, ethnicity and culture recognised by the family?
Background: What is the background to the parent’s relationship? have they been known to social care or other key agencies, what is this information. What is the nature, history of their relationships? Patterns of abuse across relationships. Have they experienced stable loving care as adults themselves or not? Have they previous children. Do both parents live with the child? If not, what contact does each parent have with the child? Is father of the child named on the birth certificate? Are there any court orders relating to the child which influence contact with either parent? What are each parent’s life story/history/background? Any criminal offences? History of involvement by any services, (mental health, substance misuse, domestic violence, criminal justice).
Health/disability: Does the parent have any physical/emotional or mental health issues, diagnosis, or specialist support from services? Are they engaged in services if this is a need? How does this issue effect their functioning/parenting? Is there any evidence of a cognitive and/or learning difficulty? History of learning difficulty at school whether or not diagnosed? It might be appropriate to approach the education service for information. Do the parents/carers have any specific health needs/disabilities and consider how these additional needs could impact their parenting?
Childhood Issues: Has the adult been known to Social Care as a child? What are their own parenting experiences? Have they experienced trauma, abuse in their own childhoods? What are or have been their attachments to wider family growing up? What is the parent’s experience of being parented? Were they brought up by their own parents or did they experience alternative carers (whether family or foster carers)? Did the parent’s upbringing involve any mental health/substance misuse/domestic violence? Are grandparents still together? Is there any history of involvement by any services? Did they experience bullying as children and what was their own experience of being at school? Did they attend a special school? Were they abused as a child? Was there any involvement from social care or other agencies? Did they observe domestic violence and abuse anywhere throughout their lives prior to becoming a parent?
Substance Misuse: Is there evidence of substance misuse? Is this accepted or denied, is insight shown into the effect and impact this has on their parenting and wellbeing/presentation. Is there evidence within the assessment that the parent has presented as under the influence, how did this affect their behaviour. Are they engaged in services of support? What information does Achieve Recovery Services hold, is there a pattern of relapse, long history of substance misuse, what may be the parents capacity/motivation to change in this area. Achieve Recovery Services Tel: 01204 557977
Violence: Is there a presentation of aggressive or violent behaviour, intimidation? Is there offending behaviour? How do the parents perceive disciplining their children? Are there regular arguments in the family home, heightened emotional responses? What may be triggers to violence? Is this escalated by drugs/alcohol? Is there a pattern of engaging in abusive or violent relationships? What are the power and control dynamics within a relationship.
Support Networks: Who is in the extended family? Who are the parent’s key sources of support? It is essential that this area is explored should longer term plans for a child require consideration to removal from parents. Consider the influence of wider social networks upon the family, including noting whether these are strengths or weaknesses e.g. does the family attend any organisations or faith groups? What is the impact of this? (There is research evidence that membership of a faith group is one of the indicators of resilience but it might also be a source of risk). Who are the adults who regularly visit the house and what are the positive/negative implications? Where is the circle of support for the child and for the family?
In this section, consider the wider influencing factors upon the family that may impact the care given to the child/young person. Consider where the strengths may lie and any weaknesses which may be indicated either through historical social care or wider agency involvement with both the identified child/young person or their family.
It is key to remember that the development and care of children does not take place in a vacuum which is unaffected by external influences. All family members are influenced, both positively and negatively by the wider family members and close friends, the neighbourhood, and culture in which they live. The history of the parents and of individual family members may have a significant impact on the child’s daily lived experiences.
History and functioning, wider family: History of the current partner if they are not the birth parent. Be clear not to miss any hidden adult which may have contact with the child. Are there any other adults in the house? Consider the potential impact upon another adult being within the family home and whether they assume any level of parenting for the child. This may be a member of the extended family, adults who come to the home to care for a disabled child or to support a parent with a learning difficulty. It is important to think about other adults living in the household in a variety of different circumstances and whether they can be viewed as a strength or potential risk (e.g. a lodger).
How did this family come together? Consider how and where did parents meet. Are there previous partners who share parenting? In what circumstances and how quickly did the child/ren arrive? What did the pregnancy/birth mean for each of the parents?
Housing: Consider the family’s stability and security within their home. How long have the family lived in the property? How many different homes has the child lived in within their life and how has that impacted peer relationships and educational opportunities? What is the condition of the property and who owns the property? What is their relationship with the neighbours/local community? What is the neighbourhood like for the family and is it appropriate for the child? Is there a safe outdoor space for the child to play? Do the family feel settled in their home? What do they like about their home and their area? What is problematic for the family in relation to their home situation? What other sources of support are there in the family/community? Also consider the wider community location upon the daily lived experience for the child. Has anyone in the family experienced physical or verbal violence? What is the pattern of such violence? Are they willing to disclose/discuss the subject?
Employment: Do parents/caregivers work? What hours does this involve? If parents work what child care arrangements are there? Are parents actively seeking work if unemployed? Are there barriers to work, incapacity? Do parents working hours impact on the child?
Income: Sources of income and how is it used and managed for the benefit of the child? Financial issues within a family can have far reaching implications for the care provided to the child, both practically and emotionally. Consider who within the household makes the financial decisions. What debts are there and how are these being managed? Who is owed money? Have the family had any money/benefit advice and are they accepting of advice? Do the family need signposting? Is either parent in employment - is this secure/casual/seasonal and how does this impact their involvement with the child? Are the parents able to provide the child with any money of their own (pocket money) or fund social activities? Are financial issues a cause of strain within the family and does the child openly witness this?
Social integration and community resources: What services are the family receiving at the moment? Consider the level of engagement from the family. Do they think they need any help or support and what is their attitude towards people and services? What has changed or is changing as a result of help?
Are there any barriers to disclosure of community issues? Does the family, both children and adults, feel safe in the house? What forms of transport are available to the family? How easy is it for the family to access facilities such as shops, getting to work, doctors and health clinics, children’s schools?
In this section, consider the use of how a parent or carer meets the needs of the child of young person by relating it to the Assessment Framework triangle as a basis. Consider how each parent provides for and responds to their child/young person’s needs and what both the strengths and weaknesses are in this area. It is often helpful to start by considering what are the specific sources of vulnerability for the child/young person in question and how could they or do they impact upon the parenting required by that child.
In summary - consider clearly whether each parent is able to meet the needs of the child and the impact of parental past experiences on their current parenting capacity, their ability to face and accept their difficulties, their ability to use support and accept help, and their capacity for adaptation and change in their parenting response. Observation and interaction is key to ensuring the professional judgement is evidence based.
Consider each parent or caregiver individually, and ensure that any potential influence on their ability to parent effectively is considered e.g. mental health issues, poor physical health, drug or alcohol misuse, domestic violence, isolation, language barrier. Ensure that a hidden partner, particularly a “hidden male”, is considered within this section of the assessment.
Basic Care and Wellbeing of the child
Is the child clean, washed and bathed regularly? Are they receiving regular meals? Are there wider concerns that the child is always presenting as hungry? Adequate nutrition provided which promotes a healthy lifestyle? Is food regularly available and healthy? Is the child attending a dentist regularly? Are the child’s medical needs attended to and in responsive timing? Describe relevant information such as diet, smoking, use of alcohol and drugs. Do people smoke in the house? Consider the impact of this if the child suffers from asthma or another breathing disorder. Has the social worker had full access to the child’s home, seen the child’s bedroom? Does the child raise any concerns or worries about their day to day care?
Ensuring the Safety of the Child
Consider if there is appropriate protection inside and outside of the house (floor coverings, electrical safety, evidence of weapons, drugs, stair gates, garden gates); Are there other adults coming into the house who may pose a risk? Use your professional observations - is it safe for a child to be living here? Are there animals? Are they companion animals or for protection? Consider that if professionals feel threatened then what is the child’s lived experience? Are the animals treated appropriately? Is there animal waste inside or outside the house? Are the children given appropriate boundaries for their age and understanding?
Emotional Warmth for the Child
What is the quality of the child - parent/caregiver relationship? Do parents respond appropriately when the child is upset or distressed? Does the parent give praise and encouragement? Do they demonstrate empathy with the child? Does the child experience age appropriate physical warmth? Does the child experience high criticism/low warmth environment?
Stimulation of the Child
Consider how each parent is able to provide interaction and stimulation to the child to encourage and promote the child reaching their full potential. Do the parents read to the child? What opportunities are there for the child to do engage in age appropriate activities? If the parent has a learning difficulty, how could this affect the child and are there others who could provide support as the child develops? Is the child’s language developing age appropriately? How does the interaction with the child help the child to learn and develop - or not?
Guidance and Boundaries for the Child
Consider whether the guidance and boundaries provided are age appropriate? Are there any routines in place for the child? How do the parents establish boundaries? What are the sanctions or rewards, and are they consistent? Are the parents able to respond to and manage the child’s behaviour appropriately and safely?
Stability for the Child
Consider how stable has the child’s life been so far - how many changes of partner or address has the child experienced? What steps has the parent taken to make the child’s life stable despite difficulty? Is there a secure attachment to the parents and how is this evidenced? Is the child attached to others within the family or close social support?
Good things about being a Parent!
Encourage and facilitate the parent to reflect upon their relationship with their child and what they mean to them. This can be especially important for parents of very young children who have not yet developed language to express views and wishes. Empower parents to consider their strengths, as well as where they can identify the need for further support.
What are Parent’s Views of the Challenges of being a Parent?
What are the parent’s expectations of their child? Are they appropriate? Sources of stress? You may want to consider using tools such as the Daily Hassles Scales.
What is the parents capacity to achieve any change and what may be their motivation to change? Do they show insight into the concerns raised?
Once you have analysed the parent’s capacity to meet the child’s needs, there should be good picture of what impact of the parents parenting style has on the child. This section should refer to any direct work undertaken with the child, including the use of research and other tools you may have used to analyse child impact. The child’s lived experience must be considered. Ask yourself what it must be like to be this child and live a day in the life of this child. Key here to include observations of the child and any direct work completed with the child. Consider how the child is presenting and in particular consider any behaviours and how this may have reflected what child has witnessed or been the subject of. What is the potential impact upon the child if the circumstances do not change and the risks are not reduced?
What does research tell us that is key within the decision making and planning for this child? Reflectively consider research and how it is specifically relevant for this family - do not just copy and paste quotes into the assessment.
Do the parents and wider family take on board the concerns raised throughout assessment?
Why are we assessing now? Summarise the major concerns, reflect the reason for assessment, has anything changed throughout the single assessment process?
What should a plan reflect - ensure the objectives are SMART. Consider the following key questions within the analysis:
- Consider using the strengths, vulnerabilities and risks framework when considering the level and outcome of analysed risk. Is this a child at risk of suffering or likelihood of suffering Significant Harm, or a Child In Need? What is your evidence to support this?
In some assessments, there may be no risk or concern, and the initial referral concerns may be unsubstantiated. In this case, the strengths will be clearly highlighted with an evidence base of why the assessment can be closed with no further action. Do not repeat descriptive information which is in the bulk of the assessment; make sense of what it means.
Managers’ roles and responsibilities are to ensure the quality of assessments, including oversight of the recommendations and planning following assessment.
Key issues for managers to remember when authorising an assessment:
- Do not move to 45 day unless triggers are met;
- Ensure that there is a clear analysis of risk in the assessment;
- No abbreviations (unless explained);
- Ensure chronologies, family, agency and any previous history is considered, and explicit within the assessment;
- Child is clearly featured in the assessment;
- Ensure child seen in a timely manner (at least before day 10).
Specific
Start by being clear about the actual significant need/risk as indicated in your assessment. Avoid clichés or describing general needs e.g. “John needs to reach his full potential “Do not describe needs in service terms e.g. “John needs to be referred to CYPMHS” this is an action not a need or identified risk. What are you concerned about. For example “John has difficulty with attention and concentration affecting his hyperactivity and ability to focus in education”. The plan should not contain a list of needs. Think why the child requires a plan; they probably did not go onto a plan because they need a dentist! However if a child is being neglected and is in urgent need of dental treatment this matter is different and should be highlighted within the plan as a significant need of the child.
Measurable
Something’s are not easily measured in numbers e.g. Jon to have 100% school attendance. Measuring whether a child is less neglected or emotionally abused is even harder. It is important here to consider the change required and the overall outcomes in which you are hoping to achieve.
Achievable and Realistic
Plans should not require parents to provide more than good enough parenting. Good enough parenting is the type of care that ‘could be reasonably expected of a parent of a similar child. This means what level of care would most children of a similar age get from a reasonable parent and how would most such children present. Realistic timescales have to be set in relation to other agency tasks and for parents to achieve, plans should not be overloaded with tasks, setting parents up to fail. Tasks should be clear to indicate who is responsible, and what needs to be achieved.
Timely
Important to set realistic timescales to ensure drift is managed, if time required is too long what are the implications for the child? Timescales must be reviewed and hopefully families should be able to see their plan shrinking demonstrating outcomes are being achieved.
- Department of Health (2000) Framework for the assessment of children in need and their families. London - The stationary Office;
- Working Together to Safeguard Children - A guide to inter-agency working to safeguard and promote the welfare of children;
- Hedy Cleaver, Ira Unell, Jane Aldgate (2011) Children’s Needs - Parenting Capacity. Child abuse: Parental mental illness, learning disability, substance misuse, and domestic violence. The Stationary Office;
- Hedy Cleaver, Corrinne Wattam, Pat Cawson and Rosemary Gordon - Ten pitfalls and how to avoid them. What research tells us (NSPCC);
- “The Munro Review of Child Protection: Final Report - A child centred system” (Cm 8062, May 2011);
- Attachment based Practice with Adults - Bain and Morrison;
- Improving safety, Reducing harm - Children, young people and domestic violence - A practical toolkit for front-line practitioners (DHSC 2010);
- The Child’s World - Jan Howarth;
- Comprehensive Guide to Assessing Child in Need - Jessica King Publishers;
- Evidence Matters in Family Justice - Research Pack - Jane Lewis and Nicola Erlen - Research in Practice Website - Copies with all teams;
- Attachment-based therapeutic interviewing manual-a practitioner’s handbook - Clark Bain and Tony Morrison 2007;
- Modified SSP for sibling assessment 1
Farnfield, S. (2009) A modified strange situation procedure for use in assessing sibling relationships and their attachment to carers, Adoption and Fostering, 33,1, pages 4-17.
Decision Making within a Child’s Timeframe:
- Tools;
- Day in the life;
- Graded Care Profile;
- 3 houses;
- Department of health questionnaires and scales.
Last Updated: June 3, 2024
v30
